
 PERIANAL ABSCESS:
PERIANAL ABSCESS:
Formation of abscess is a very common ailment occurs in all over the body. When it happens into the surroundings of anal region it is called a perianal abscess.
INCIDENCE :
This is more common in male than female and probable ratio is 2:1 and more common in young and middle aged person.
ETIOLOGY :
It is believed that infection from an anal crypts via an and gland plays the major role in causation of a perianal abscess.
This can also occur secondary to following conditions.
- Fissure in Ano – Particularly dorsal fissure
- Bursted anal heamatoma
- Prolapsed thrombosed internal haemorrhoids
- Pruritis Ani
- Trauma or any other Anorectal surgeries
- Injection therapy in haemorrhoids
- Trauma or any other ano-rectal surgeries
ORGANISMS FOUND IN ABSCESS.
- Staph. Aure – Predominantly
- Streptococci, E-Coli, or Prosteus Supp.
- Clostridium Welchii
- Mixed Infection
ADDITIONAL FACTORS :
- Tuberculosis
- Ulcerative Colitis
- Crohn’s Disease
- HIV – AIDS
CLASSIFICATIONS :
- Perianal
- Ischiorectal
- Submucus
- Pelvirectal
- Atypical
FEATURES :
- Pain – Throbbing
- Swelling
- Tenderness
- Fever
- Spontaneous discharge – Relieves the pain.
INVESTIGATIONS :
CBC, FBS, PLBS, Urine Rt etc.
Ultrasonography, CT Scan, MRI etc.
TREATMENT :
- Self medication is absolutely contra indicated in cases of perianal abscess.
- Proper Hygienic conditions and antibiotics may solve the problem in some cases.
- But majority of the cases needs proper incision & drainage treatment.
- Whenever surgeon feels that this abscess is tends to fistula in ano needs complete laying open of the tract.
- The Abscess which are leading to Fistula-in-Ano can be treated with Ksharasootra at the same time.
- In spite of proper incision and drainage treatment it relapses so treat such cases with ksharasootra treatment, helps in preventing the recurrence of the diseases.
 FISSURE IN ANO
FISSURE IN ANO
This is the commonest condition of anal region. Simple split in the skin of the anal canal or an elongated ulcer in the long axis of the lower anal canal is called fissure in ano.
Incidence : Usually it occurs in young or middle aged adults and equally affects to both the sexes i.e. male & female.
Site :
- Mid Line Posteriorly
- Mid Line Anteriorly
AETIOLOGY:
- Exact patho physiology is not known and mainly it is based on speculation. It seems that trauma to the anal canal during the passage of a large hard motion is generally responsible for the causation of the disease.
- Some believes that sharp curve of posterior wall of rectum from sacrum to anal canal is responsible for the causation of this condition.
- Regular use of laxative taking person suddenly passes hard stool.
- Spasm of sphincter makes it chronic.
- Secondary to post anal surgery.
- Procto Colitis, Ulcerative Colitis, Crohn’s disease.
PATHOLOGY :
- Usually it occurs midline posterisaly.
- Antorior is common in woman, 10% female/1% male.
- Occasionally they are multiple in numbers.
- Deep Fissures extends upto internal sprinetar
SECONDARY CHANGES
- It is believed that Fissure gives excruciating pain and to come out of this pain body itself makes certain changes & i.e. sentinel piles or skin tag.
- Hypertrophied papilla or polyp.
- Perianal Abscess.
- Spasm or Contraction.
SYMPTOMS :
- Pain – Sharp, Cutting, Tearing, Burning
- Bleeding - Usually streak with the stool or few drops
- Swelling –
- Discharge and pruritus Ani
- Urinary Symptoms like – Dysurea, Retention & frequency.
DIFFERENTIAL DIAGNOSIS :
It must be differentiated from other anal conditions like
- Syphilis
- Tuberculosis
- Ulcerative Colitis
- Cancer
- Crohn’s Diseases.
TREATMENT :
Conservatives :
Superficial Fissures, heals spontaneously within 2 to 3 weeks but one must take proper precautions i.e.
- Proper dosage of laxative as per the advice of doctor
- Hot Water Seitz bath
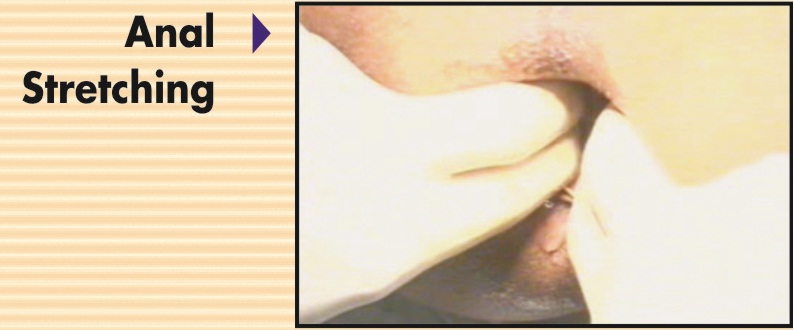
- Anal Dilators
- Some healing agents for local application.
SURGICAL
- Anal Dilatation : Manual dilatation of and canal under proper anestheasia. This procedures is also known as lord’s procedure.
- Sphincterotomy : Just simple division of internal sphincter muscle.
- Mainly either of these two procedures are performed and occasionally fissurectomy or fissurectomy with immediate skin grafting is performed.



HAEMORRHOIDS - PILES
This is one of the most common ailment people suffers during their life span and sometimes it can be fatal also if not taken care of.
The word haemorrhoid is a Greek word comprised of two words
I)Haima – Blood
II)Rhoos – Flowing
Thus, the disease in which blood flows is known as haemorrhoid.
Secondly the word piles is a Latin name derived from pila i.e. ball means the disease in which the abnormal structure grows like a ball is called piles.
INCIDENCE :
As age progress higher the rate of incidence of the disease. Further current dietary habits, increases the incidences. Various text quotes 50% to 70% of incidence during the life span. It affects both male & female equally.
Haemorrhoid or piles is commonly occurs because of engorgement or varicocity of Anal/Rectal veins. These veins do not have valves they are prone to engorge or swell whenever the pressure come on to it due to various reasons like, constipation & straining, pregnancy etc.
SYMPTOMS :
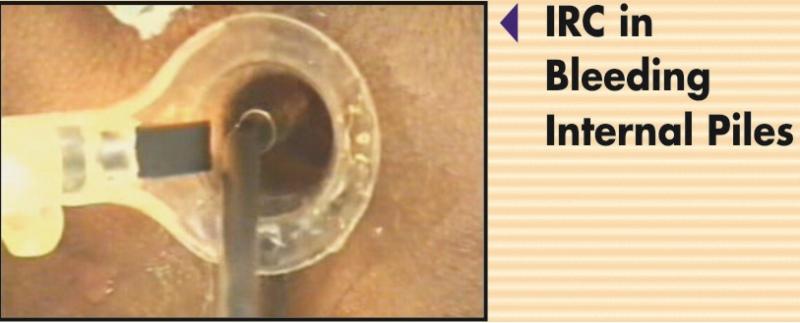
BLEEDING P/R
i)Generally it is bright red in colour
ii)Profuse or drop wise
iii)Association of Pain could be because of ext. piles, int. piles are having generally painless bleeding.
PROLAPSES :
From 2nd degree onwards pile protrudes
DISCHARGE :
III & IV degree piles may have mucous type of discharge.
ANAL IRRITATION :
Mass as III & IV with discharge causes irritation.
OTHER SYMPTOMS :
a) Loss of Appetite
b) Borborygum
c) Belching
d) Anaemia
e) Distension of Abdomen
f) Breathlessness
g) Weakness etc.
ETIOLOGY :
1) Constipation & Straining
2) Diarrhoea
3) Pregnancy
4) Abdormiral Tumours
5) Heredity
6) Obesity
7) Sydentary Lifestyle
8) Diet & Lifestyle
Now a days diet & lifestyle plays an important role in causation of Ano-Rectal Diseases.
TYPES :
1)External : Generally this occurs at a lower one third of the anal canal or at the anal orifice itself.
2)Internal : Generally this occurs n upper two thirds of the anal canal which is lined by columnar celled epithelium.
NUMBERS & POSITION :
Int. piles are three in general and are located at 3, 7 & 11 O’clock position.
DEGREES :
This depends on the size of the mass – and is classified as under
1)Ist Degree : Hardly they are visible into lumen & never comes out of the anal canal.
2)2nd Degree : It comes out and goes back spontaneously.
3)3rd Degree : It comes out but does not go back into it by it’s own. It has to be replaced manually
4)4th Degree : Normaly long standing piles with skin component does not go inside and remains as a permanent projection of Anal mucosa.
So, this completely irreducible piles are known as a forth degree piles.
COMPLICATIONS :
If the conditions is not treated it leads to several complications like :
a)Profuse Bleeding
b)Thrombosis
c)Ulceration
d)Gangrene
e)Fibrosis
f)Suppuration
g)Pylephlebitis
DIFFRENTIAL DIAGNOSIS :
Before coming to final conclusion of treatment of piles one must rule out following conditions :
(1)Ulcerative Colitis
(2)Crhon’s Disease
(3)Rectal Polyp
(4)Fistula in Ano
(5)Cancer
TREATMENT :
MEDICAL MANAGEMENT :
A)Laxative, Stool Softorner
B)Heamostatic
C)Anti inflammatory
D)Antibiotic – as & when required
E)Seitz Bath – Hot Water Bath
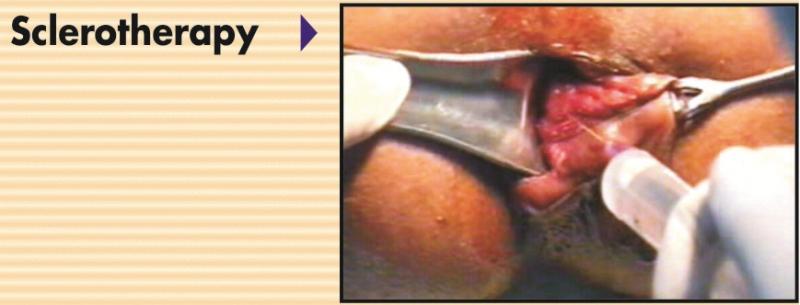
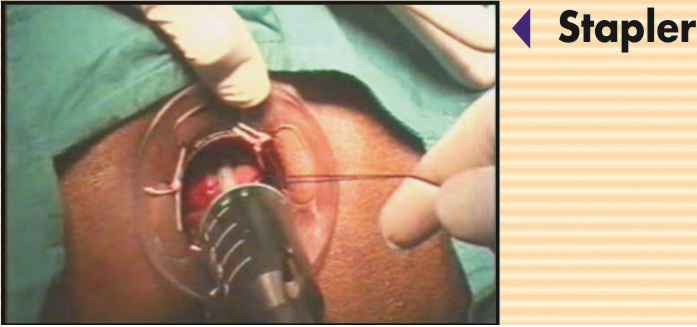
All these helps in relieving signs & symptoms of the disease & can be used for 1st degree piles & in some cures 2nd degree piles. Even than some times it does not responds to 1st & 2nd degree piles also. So various surgical and parasurgical modalities are available to treat the disease piles – which is described in detail various surgical procedures see complete details of piles surgery.
ABOVE ALL
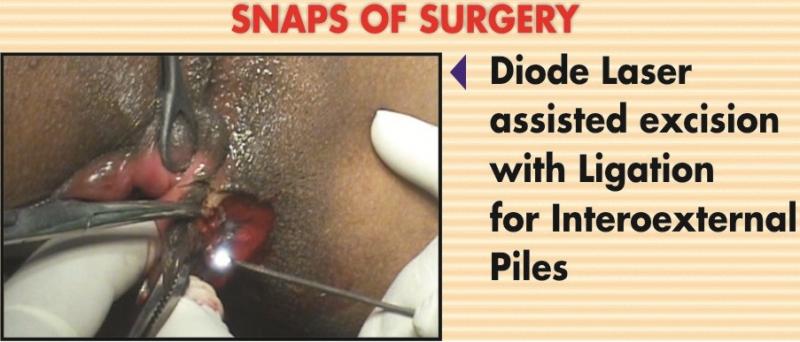
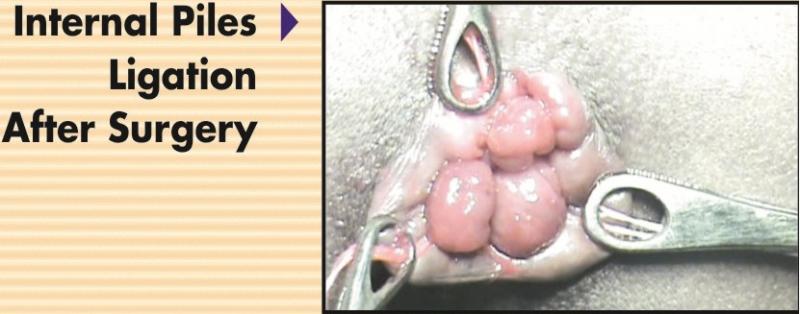
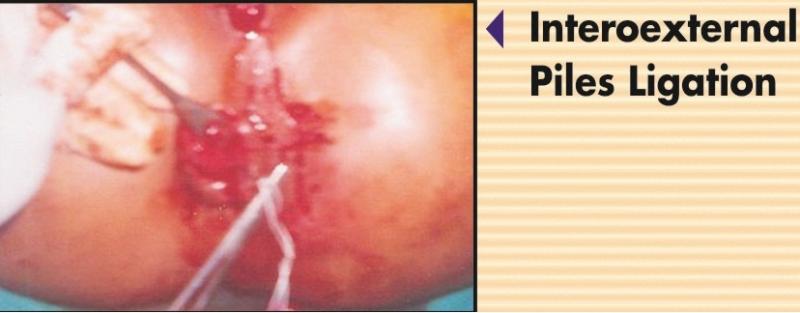
In India we used to do simple Ligation with plain barber linen thread No. 30 or with medicated seton i.e. Ksharasootra. It has got various advantages over conventional surgery which is narrated below.
From the table you can see that pain factor is more in Int., Ext. Piles treatment with ligation in such cases diode laser assisted ligation gives excellent result and we recommend strongly either plain ligation or diode laser assisted surgery becauses of it’s various advantages

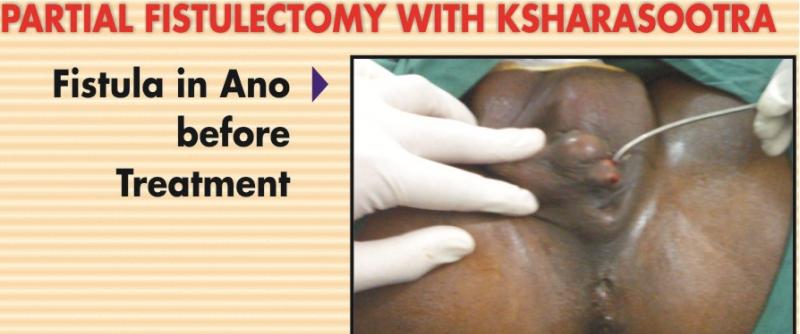
FISTULA-IN-ANO
Definition :
A fistula in Ano is a track, lined by granulation tissue which opens deeply in the anal canal or rectum and superficially on the skin around the anus.
But many a times it is complicated and is having multiple external openings and is having ramification of main track also.
GENERAL INFORMATION :
The term SINUS means bay or recess in Latin and is taken to mean a granulating track which is open at only one end. Whereas the the team Fistula means a reed, pipe or flute in latin which is having a opening at both the end in track. But In case of such sinuses in perianal region it is considered as a blind fistulae.
INCIDENCE :
This is a conditions of a young people and predominantly of a men. Overall male/female ratio is roughly 5:1.
TYPES :
I a)HIGH ANAL : Fistula track which is having an internal opening in between the pectinate line to just below the ano rectal ring.
b)LOW ANAL : In these Fistulae generally it opens at a level of anal crypts, at a level of pectinate line.
II a) Subcutaneous
b) Sub Mucus
c) Low Anal
d) High Anal
e) Pelvi Rectal
III a) Intersphincteric
b) Trans Sphincteric
c) Supraleavator
Importance of type of Fistula & Ksharasootra :
Fistula in Ano is a condition where there is very a high recurrence rate inspite of doing the surgery. In this conditions the structure of ano – rectal region like sphincters, supralevator muscle etc. plays a very important role in the continence (i.e. : Control over Flatus, Facess, etc.) one has to take care during the excision of these structure otherwise the patient may landup with permenant incontinence and that is where the role of seton – medicated thread i.e.: Ksharasootra comes in which is very helpful in preventing recurrence as well as incontinence. Information of Ksharasootra is given on the separate page.
CAUSES :
- Previous pyogenic Abscess
- Fish bone, Egg shell
- Blood Borne infection
In a simple words we can say that this is a infectious disease. In which Anal valves, Anal Crypts and Anal duct’s infection plays an important role because of the above written causes :
Bacteria comes in blood stream from any source and lodges into this area, impaction of foreign body like fish bone or egg shell or previous ano-rectal abscess infect the anal structures as mentioned above plays an important role in causation of Fistula-in- Ano.
There are conditions also which plays an important role in causation of Fistula in Ano are as under :
- Tuberculosis
- Ulcerative Colitis
- Crohn’s Disease
- Ca – Rectum
- Previous Ano Rectal or Gynecological Surgery.
SIGNS & SYMPTOMS :
- Sero purulent or purulent discharge
- Swelling in the perianal region
- Fever
This can be persistently or intermittently.
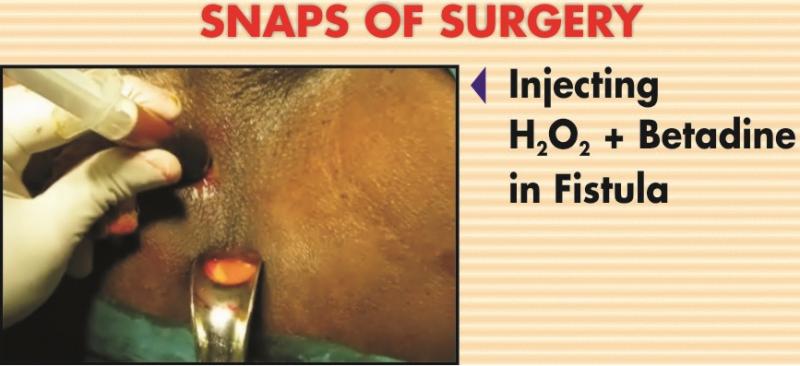
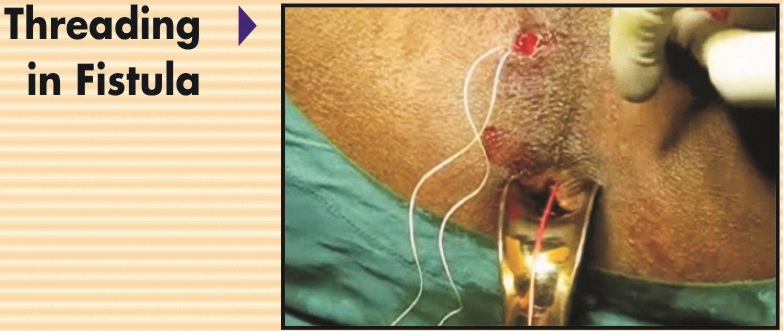
TREATMENT :
- Fistulotomy
- Fistulectomy
- Coring of track
- Laying open of the track with primary structure
- Loop
- Plain Seton
- Ksharasootra
- Partial Fistulectomy with Ksharasootra treatment. The role and importance of Ksharasootra has been described under the head of Kshaasootra Chapter whereas the comparative study table is given below :

.jpg)
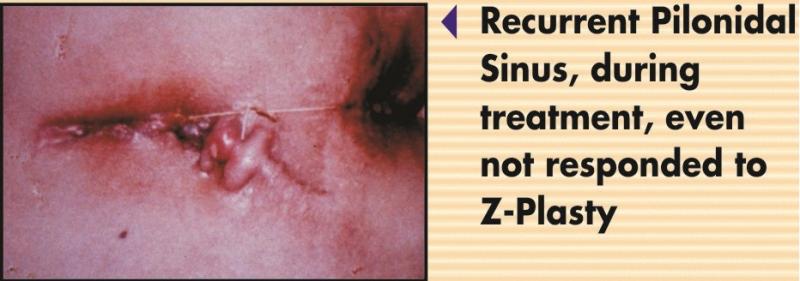
PILIONIDLE SINUS :
Before narrating this condition, this is for your information that this centre and it’s doctor, Dr. Nilesh B. Doshi is a pioneer in designing it’s treatment under the head of minimal sinusectomy with Ksharasootra application with excellent result since 1994. And has presented his work at various places in India.
DEFINITION :
The term Pilonidal Sinus compraised of two words
a) Pilus = Hair
b) Nidus = Nest
Thus the diseases where you finds a nest of hair is a called pilonidal sinus.
HISTORY :
- In 1847, Mr. Anderon, extracted the hair from an ulcer.
- In 1854, warren snow an abscess in natal region which was containing hair
- In 1880, Hodges coined term pilonidal sinus.
SITE OF THE DISEASE :
1)Most commonly Post Anal or Anococcygeal (most commonly) i.e. approximately 5 cms. Above the anus in the mid line.
2)Other sites of the disease
- Finger web of barber
- Axilla
- Perineum
- Umbilicus
- Suprapubic
INCIDENCE :
Normally this is a disease of very young people of say about 20 to 25 years and is predominant in hairy male. It also occurs in obese and blond people too.
CLINICAL FEATURES :
Generally first abscess is formed in the natal region which either burst opens on its own or by the doctor than it discharges the pus, the discharge may ceases after few days. Later on nodule of induration or pin hole opening is left behind. If this is not treated radically this process keeps on going on and off than it may have a series of opening, projection of hair in these openings and many a times it may have a secondary opening – majority of the time it is in the left side. In acute condition patient may have a fever also.
PATHOLOGY :
- The Preengland Theory
- The Medullary Canal Vestige Theory
- The Traction Dermoid Theory
- The Inclusion Dermoid Theory
- Acquired Conditions
It is majorly considered as an acquired disease in which surrounding natal hairs penetrates the soft tissue which ultimately creates the nest of hairs in natal region which gets infected and causes the disease pilonidal sinus.
INVESTIGATIONS :
Sinogram and MRI are useful tool to know the course and extent of the disease.
TREATMENT :
- Complete Execision of the Sinus
- Primary Suturing
- Z-Plasty
- Minimal Sinectomy with Ksharasootra application i.e. Medicated Seton.
Ksharasootra treatment is giving the best result for this condition and comparative table of the same has been given above.




A recto-vaginal fistula - as the name indicates is a fistula, an abnormal connection between the rectum & vagina. The opening between the rectum & the vagina will allow the passage of faeces or flatus (gas) from the rectum to the vagina, creating an unhygienic, embarrassing and stressful condition for the patient. Not only there may be flatus and faecal matter being discharged / leaking out of the vagina, but it may lead to recurrent urinary and vaginal infections.
Recto-vaginal fistula can develop in women, young girls who are victims of forced sex. However, the most common cause found in women specially of developing and underdeveloped countries (in conditions where there is inadequate health care), is trauma during child birth r infection or tear of an episiotomy. This type of recto-vaginal fistulas is termed as “Obstetric fistula”. The cause may be tears in the perineum that extend to the bowel, following a long & difficult labour. Obstetric fistula may involve injury to the anal sphincter also – this making matters more serious.



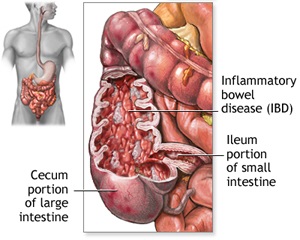
Crohn's disease (also spelled Crohn disease) is a chronic inflammatory disease of the intestines. It primarily causes ulcerations (breaks in the lining) of the small and large intestines, but can affect the digestive system anywhere from the mouth to the anus. It is named after the physician who described the disease in 1932. It also is called granulomatous enteritis or colitis, regional enteritis, ileitis, or terminal ileitis.
Crohn's disease is related closely to another chronic inflammatory condition that involves only the colon called ulcerative colitis. Together, Crohn's disease and ulcerative colitis are frequently referred to as inflammatory bowel disease (IBD). Ulcerative colitis and Crohn's disease have no medical cure. Once the diseases begin, they tend to fluctuate between periods of inactivity (remission) and activity (relapse).
Inflammatory bowel disease affects approximately 500,000 to two million people in the United States. Men and women are affected equally. Americans of Jewish European descent are 4 to 5 times more likely to develop IBD than the general population. IBD has historically been considered predominately disease of Caucasians, but there has been an increase in reported cases in African Americans suffering from IBD. The prevalence appears to be lower among Hispanic and Asian populations. IBD most commonly begins during adolescence and early adulthood (usually between the ages of 15 and 35). There is a small second peak of newly-diagnosed cases after age 50. The number of new cases (incidence) and number of cases (prevalence) of Crohn's disease in the United States are rising, although the reason for this is not completely understood.
Crohn's disease tends to be more common in relatives of patients with Crohn's disease. If a person has a relative with the disease, his/her risk of developing the disease is estimated to be at least 10 times that of the general population and 30 times greater if the relative with Crohn's disease is a sibling. It also is more common among relatives of patients with ulcerative colitis.

Constipation is a condition familiarly to all young sold. There is no every child or adult, who has never experienced this condition. Though the reviarity may other.
Constipation usually is attributed to faulty food habits & improper off style. Though a number of medical conditions are known to cause constipation the must common cause are lers constipation of fiber & fluid.




Genital warts, also known as condylomata acuminata or venereal warts, are one of the most common types of sexually transmitted diseases. New genital wart infections affect about 5.5 million Americans each year.
As the name suggests, genital warts affect the moist tissues of the genital area. They may look like small, flesh-colored bumps or have a cauliflower-like appearance. Sometimes they may be only 1 to 2 millimeters in diameter. In other situations, the warts may multiply into clusters, which can be quite large.
In women, genital warts can grow on the vulva, the walls of the vagina, the area between the external genitals and the anus (perineum), and the neck of the uterus (cervix). In men, they may be found on the tip or shaft of the penis, the scrotum or the anus. They can also develop in the mouth or throat of a person who has had oral sexual contact with an infected person.
Although genital warts can be treated, they are a serious health concern. The virus that causes them - the human papillomavirus (HPV) - has been associated with cervical cancer. It has also been linked with other types of genital cancers.
 This is itching or irritation of the perianal area and it occurs as a symptom of many conditions. The commonest cause is irritation of the skin caused by moisture of faecal soiling. Also some primary skin diseases or perianal conditions can cause irritation.
This is itching or irritation of the perianal area and it occurs as a symptom of many conditions. The commonest cause is irritation of the skin caused by moisture of faecal soiling. Also some primary skin diseases or perianal conditions can cause irritation.
Anal itch is an intense itching around your anus - the 1 1/2-inch-long canal that's the outlet for your rectum. It can be an embarrassing and uncomfortable situation. The itch, located in your anus or on the skin just around your anus, may be accompanied by a strong urge to scratch.
Also called Pruritus ani, anal itch has many causes. Numerous factors may cause anal itch to be more intense - including moisture, the abrasion caused by your clothing, and the pressure of sitting. Anal itch is usually most noticeable and bothersome at night or right after a bowel movement.
Anal itch is a common problem that most people have experienced. Don't be afraid to talk with your doctor about this condition. With proper treatment and self-care measures, most people can achieve complete relief.

 Anal stenosis is the most common type of outflow obstruction and is usually mistaken for constipation. It is the second most frequently missed anal diagnosis. This is unfortunate because it can be treated very easily in the office under local anesthetic. The symptoms are difficulty pushing a firm stool through a narrowed Anal canal. It comes on slowly so the patient is not fully aware of the narrowing nd attributes it to "constipation". The problem is that the anal canal has been narrowed by a ring of scar tissue located just under the skin of the anal margin which, just like a bone, will not give or allow the anal canal to stretch to accommodate a large diameter stool.
Anal stenosis is the most common type of outflow obstruction and is usually mistaken for constipation. It is the second most frequently missed anal diagnosis. This is unfortunate because it can be treated very easily in the office under local anesthetic. The symptoms are difficulty pushing a firm stool through a narrowed Anal canal. It comes on slowly so the patient is not fully aware of the narrowing nd attributes it to "constipation". The problem is that the anal canal has been narrowed by a ring of scar tissue located just under the skin of the anal margin which, just like a bone, will not give or allow the anal canal to stretch to accommodate a large diameter stool.
The treatment is very simple : in the office under local, the ring of scar tissue is incised on both sides through the anal skin which immediately allows the canal to expand to its normal stretchable diameter. We recommend that a dilator be used afterwards to allow the canal to heal in the stretched position.
Rectal bleeding is a sign that something is wrong. It is usually something minor that can be easily diagnosed, but not always. It is, therefore, important that the specific cause of rectal bleeding be identified so appropriate treatment can be started and the problem corrected. Even though rectal bleeding may not be serious, an individual should never assume this to be the case. Most importantly, rectal bleeding may be a sign of rectal cancer.
Rectal bleeding always means that there is a problem. It is usually not a serious problem, but it should always be assumed to be serious until proven otherwise. The diagnosis is easy to make and effective treatment is almost always available.
 Irritable bowel syndrome (IBS) is a common gut disorder. The cause is not known. Symptoms can be quite variable, crampy pain, gassiness, bloating, and changes in bowel habits. Some people with IBS have constipation (difficult or infrequent bowel movements); others have diarrhea (frequent loose stools, often with an urgent need to move the bowels); and some people experience both. Sometimes, the person with IBS has a crampy urge to move the bowels but cannot do so.
Irritable bowel syndrome (IBS) is a common gut disorder. The cause is not known. Symptoms can be quite variable, crampy pain, gassiness, bloating, and changes in bowel habits. Some people with IBS have constipation (difficult or infrequent bowel movements); others have diarrhea (frequent loose stools, often with an urgent need to move the bowels); and some people experience both. Sometimes, the person with IBS has a crampy urge to move the bowels but cannot do so.
Through the years, IBS has been called by many names -- colitis, mucous colitis, spastic colon, spastic bowel, and functional bowel disease. Most of these terms are inaccurate. Colitis, for instance, means inflammation of the large intestine (colon). IBS, however, does not cause inflammation and should not be confused with another disorder, ulcerative colitis.
The cause of IBS is not known, and as yet there is no cure. Physicians call it a functional disorder because there is no sign of disease when the colon is examined. IBS may cause discomfort and distress; however, IBS does not cause permanent harm to the intestines and does not lead to intestinal bleeding of the bowel or to a serious disease such as cancer. Most people with IBS are able to control their symptoms through lifestyle modifications and sometimes medications prescribed by physicians. Following a special diet and stress management also can help to control symptoms.
IBS has not been shown to lead to any serious, organic diseases. No link has been established between IBS and inflammatory bowel diseases such as Crohn's disease or ulcerative colitis. IBS does not lead to cancer. Some patients have a more severe form of IBS, and the pain and diarrhea may cause them to withdraw from normal activities. These patients need to work with their physicians to find the best combination of medicine, diet, counseling, and support to control their symptoms.



Polyps are one of the most common conditions affecting the colon and rectum, occurring in 15-20 percent of the adult population. Although most polyps are benign, the relationship of certain polyps to cancer is well established.
Most polyps are not dangerous. Most are benign, which means they are not cancer. But over time, some types of polyps can turn into cancer. Usually, polyps that are smaller than a pea aren't harmful. But larger polyps could someday become cancer or may already be cancer. To be safe, doctors remove all polyps and test them.
.jpg)

.jpg)
Rectal prolapse (rectal procidentia) refers to a medical condition where a section of the wall of the rectum prolapses(falls down) from the normal anatomical position with associated pelvic floor dysfunction. This may occur while straining to defecate, or during rest.
Used unqualified, the term rectal prolapse often is used synonymously with complete rectal prolapse (external rectal prolapse), where the rectal walls have prolapsed to a degree where they protrude out the anus and are visible outside the body. However, most researchers agree that there are 3 to 5 different types of rectal prolapse, depending on if the prolapsed section is visible externally, and if the full or only partial thickness of the rectal wall is involved.
Rectal prolapse may occur without any symptoms, but depending upon the nature of the prolapse there may be mucous discharge (mucus coming from the anus), rectal bleeding, degrees of fecal incontinence and obstructed defecation symptoms.
Rectal prolapse is generally more common in elderly women, although it may occur at any age and in both sexes. It is very rarely life threatening, but the symptoms can be debilitating if left untreated. Most external prolapse cases can be treated successfully, often with a surgical procedure. Internal prolapses are traditionally harder to treat and surgery may not be suitable for many patients.
 This is a common anal complaint that is usually due to an anal problem or to poor anal hygiene. A doctor will want to know what the discharge looks like (i.e. is it faeculent, watery, mucus or pus), whether there are any other symptoms and how long it has been going on. If there are symptoms of bleeding and prolapse (something coming down and out of the anus) then it may well be due to piles. There may be associated pruritus ani (itching) due to the discharge causing damage to the perianal skin.
This is a common anal complaint that is usually due to an anal problem or to poor anal hygiene. A doctor will want to know what the discharge looks like (i.e. is it faeculent, watery, mucus or pus), whether there are any other symptoms and how long it has been going on. If there are symptoms of bleeding and prolapse (something coming down and out of the anus) then it may well be due to piles. There may be associated pruritus ani (itching) due to the discharge causing damage to the perianal skin.
Possible causes of a discharge include poor anal hygiene, piles, anal fissure, perianal abscess, fistula-in-ano, anal warts, and anal cancer. Also disease in the rectum may also cause this symptom, such as solitary rectal ulcer, an adenoma (benign growth) and Crohn's disease.
When seen by a doctor he will want to examine the perianal skin and examine the anus with a gloved finger. He may also take a sample of the lining of the rectum through a telescope in order for the laboratory to determine whether there is any inflammation of the rectum.
The treatment obviously depends on the cause of the condition.
The doctors will arrange for further tests and investigations if appropriate.
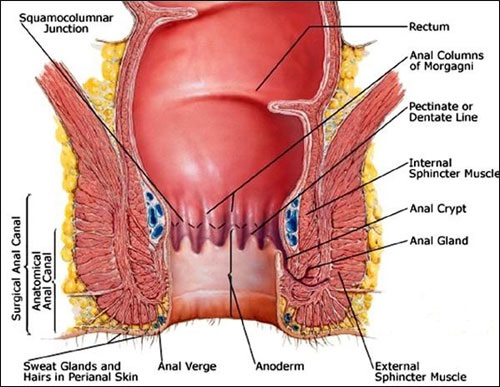
 Anal crypts are tiny recesses of epithelium at the upper end of the anal canal at the mucocutaneous junction. They are tiny mucus glands of lubrication arranged in a circle around the upper end of the anal canal. Located between normal structures called anal papillae, crypts are usually small, but visible enough to help give the pectinate line a serrated appearance on anoscopy.
Anal crypts are tiny recesses of epithelium at the upper end of the anal canal at the mucocutaneous junction. They are tiny mucus glands of lubrication arranged in a circle around the upper end of the anal canal. Located between normal structures called anal papillae, crypts are usually small, but visible enough to help give the pectinate line a serrated appearance on anoscopy.
Crypts are normal structures causing no symptoms unless they become inflamed. They are small areas of skin situated between the anal papillae. They are approximately 3 mm in depth and are lined with a single layer of epithelium, which is a continuation of the skin of the anus. Just before a bowel movement, the sphincter muscles contract and squeeze out a little drop of lubricating mucus from each of these crypts, aiding in the normal slippery passage of stool.
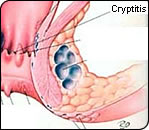
Cryptitis is defined as an inflammatory process in the crypts, characterized by redness, swelling, and thickening of the tissues in this area. This condition is identified proctoscopically as a pearl of pus beading up from the crypt at the level of the dentate line. Cryptic infection often causes the dissolution of the roof of the crypt, resulting in anal fissure. An infected crypt that is chronic, and fails to un-roof, can develop into an anal abscess and/or fistula.
Cryptitis is held responsible for a variety of conditions and symptoms. The pain of cryptitis is usually of the sharp lancinating or burning variety. A dull ache, or intense pain from spasm of the contraction of the sphincter muscle may develop from the inflammatory process. The nature of a crypt infection is of an ebb and flow, and may be of such a low grade that the pain is transitory.
The cause of cryptitis may be due to an inflammatory process in the adjacent areas, or a disturbance in the acid ph balance of the rectum. Trauma from constipated stools, infections introduced from external sources, parasites, foreign debris, etc., may also initiate cryptitis.
Surgical removal of a crypt is not the complete answer to treating cryptitis. The cause must be eliminated.
.jpg)
.jpg)
.jpg)
.jpg)

Anorectal cancer (anal cancer) is a disease in which cancer cells grow in the tissues of the anus. It is rare, with approximately 5,000 Americans being diagnosed with this cancer each year.
Symptoms
Symptoms of anal cancer include bleeding from the rectum or anus, pain or pressure in the region surrounding the anus, an itching or discharge from the anus, a lump in the region, and a change in bowel habits. Other conditions may also cause these symptoms, so it is important to check with a physician if you have any of these symptoms.
Risk Factors
Risk factors for anal cancer include infection with human papillomavirus (HPV; including strains that cause anal or genital warts), infection with HIV/AIDS, use of certain medications after organ transplantation, anal intercourse, multiple sex partners, tobacco use, and being over age 50. Frequent anal soreness, redness, and inflammation, or having anal fissures increases the risk as well.
Diagnosis
Diagnosis is based upon physical examination and a full medical history. The examination may include a digital rectal examination, anoscopy or proctoscopy to examine the anus and lower rectum, ultrasound, and colonoscopy to evaluate the rest of the colon. Finally, a biopsy may be taken to check for cancer if an area appears abnormal.
Treatment
The treatment for anorectal cancer depends on the stage of cancer, and may involve radiation therapy, chemotherapy, and/or surgery. Chemotherapy and radiation are generally the first line of treatment for anal cancers. Radiation may be administered externally or internally using radioactive seeds or catheters placed in or near the cancer. Surgery for small, contained cancer or cancer in the lower part of the bowel is usually done as a local resection, in which diseased tissue is removed along with some surrounding healthy tissue. This procedure can preserve sphincter muscles.
For more extensive cancer, a resection is performed, in which the anus, rectum, part of the lower colon, and lymph nodes are removed. The surgeon then attaches the end of the intestine to an opening, called a stoma, made in the abdomen where stool collects in a bag attached to the outside of the abdomen.